63 year old male patient was diagnosed with cancer of upper part of stomach. Patient was fit for a curative surgery on investigations. However a staging laparoscopy (endoscopy of the abdominal cavity – a type of surgery prior to main surgery) revealed a solitary deep seated lymph node spread even missed by PET-CT scan. An intraoperative frozen section histopathology (rapid test) confirmed the cancer in the lymph node. A chemoport (special system for delivering chemotherapy to avoid the trouble of searching patent veins) was inserted during the same surgery. Chemoport insertion is a surgery done regularly for patients in need of chemotherapy. Patient received 8 cycles of chemotherapy and then underwent a repeat PET-CT scan to confirm absence of metastasis. Complete stomach (including cancer bearing part) along with draining lymph nodes (lymphadenectomy) was removed successfully 4 weeks after the last cycle. A gap of 4-6 weeks is mandatory between chemotherapy cycle and major surgery to reduce risk of postoperative complications. He was put back on chemotherapy 6 weeks after the surgery and received 6 more cycles. Patient is fit and alive for 1 & ½ years since surgery.
Cancer of the stomach is a common cancer of gastrointestinal tract after colon / rectum. It often presents in an advanced stage since there isn’t any simple screening test and symptoms are often vague (vague abdominal discomfort / dyspepsia / burning) & misconstrued as ACIDITY. Endoscopy as a regular screening test is performed in country like Japan. However this is expensive in India. This leads to often delayed diagnosis when patient presents with symptoms like weakness, vomiting, weight loss, abdominal pain, abdominal lump, bleeding (in vomitus -fresh- or stool-black stools), abdominal distension (due to ascites—water accumulation or disease spread in the abdomen—peritoneal metastasis). Hence acidity in an elderly person should always be taken very seriously unless it is obviously due to some drugs like painkillers.
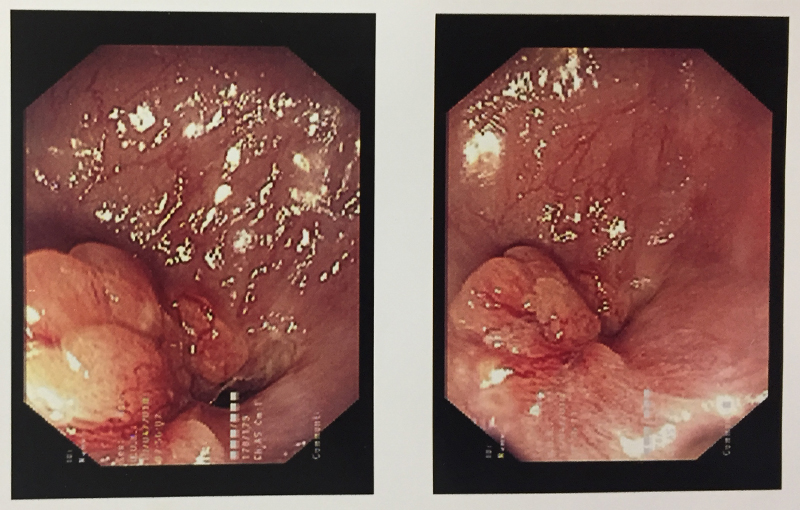
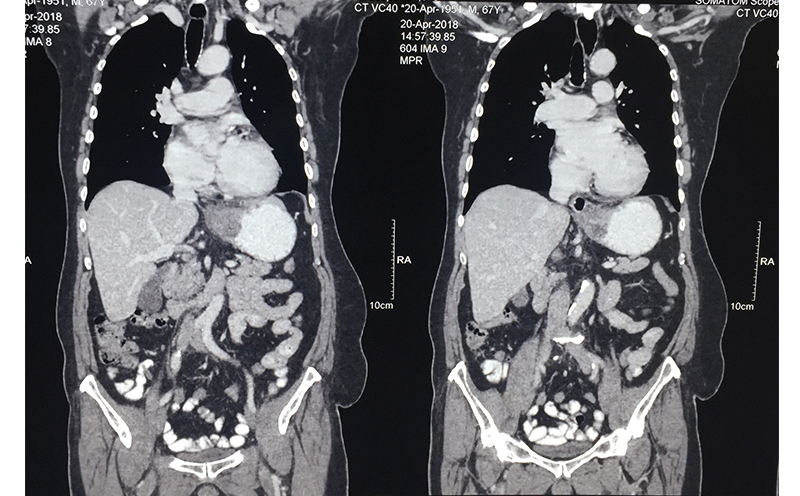
When a stomach cancer is suspected in any patient, he/she is subjected to an endoscopy of the stomach (internal visualization). This helps in diagnosis and taking a biopsy for confirmation. A CT scan is performed after the confirmation (though often patients come with a CT scan diagnosis) to see whether the cancer can be removed surgically. A PET-CT is performed prior to any therapy to see the spread / extent / stage of the disease. If the tumor is in early stage, stomach (part / full depending on which part of stomach is involved and extent) along with the tumor and surrounding lymph nodes is removed and small intestine is joined with the proximal stomach or esophagus. If the tumor is small and lymph node spread is less, this operation is done laparoscopically. A chemoport may also be placed at this time for postoperative chemotherapy (adjuvant) unless it is a very early stage disease. Very early stage cancer can sometimes be removed through an endoscopic procedure (endoscopic mucosal resection --EMR / endoscopic submucosal dissection – ESD) under the guidance of an endoscopic ultrasound equipment. Unfortunately this is very rarely possible in Indian patients since disease is advanced by the time it is diagnosed.
If the disease is diagnosed at a stage where it is advanced in the stomach walls and surrounding region with large lymph nodes then a preoperative (neoadjuvant) chemotherapy is given to downstage the disease. If this attempt is successful and tumor responds, then in that case a curative surgery is done. This is followed by further chemotherapy cycles. Occasionally external radiotherapy is given too. This kind of multidisciplinary treatment plan was used in the above case.
Multidisciplinary care involves aggressive chemotherapy to downstage the disease (inoperable & / or unresectable to operable & resectable). It is followed by a curative surgery where possible. Surgery is again followed by multiple cycles & lines (1st line, 2nd line etcetera) of chemotherapy. It is especially useful in young fit patients with aggressive cancer disease. These patients can withstand the demanding nature of this treatment regime. Good survival benefit is observed.
Patients, who undergo a successful surgery are later regularly followed in the OPD once every 3 months with baseline blood investigations and an abdominopelvic sonography. There is no blood / serum tumor marker for stomach cancer. An intermittent CT / PET-CT / endoscopy is performed depending on the need.
Patients, who have undergone a gastrectomy (removal of stomach) may experience multiple complaints in the delayed postoperative period due to the altered anatomy, bile easily refluxing into the esophagus / remnant stomach and food getting delivered in the small intestine directly. Most of them can be controlled with medications.
If the disease is advanced in the in the abdomen and / or spread to organs like liver, then patient is given aggressive palliative chemotherapy if patient is fit as we have done in some patients. Few patients will respond in a impressive manner and are able to undergo surgery that involves removal of stomach, omentum, lymph nodes, peritoneal lining etcetera. Sometimes intraabdominal chemotherapy (HIPEC) is given too. This is again followed by systemic chemotherapy. It has shown good merit in some well selected patients. However this is still a more of palliative effort and only improves survival to an extent, and will not necessarily cure the patient. Also such treatment is very expensive, has significant surgical morbidity (complication risk) and risk to life.