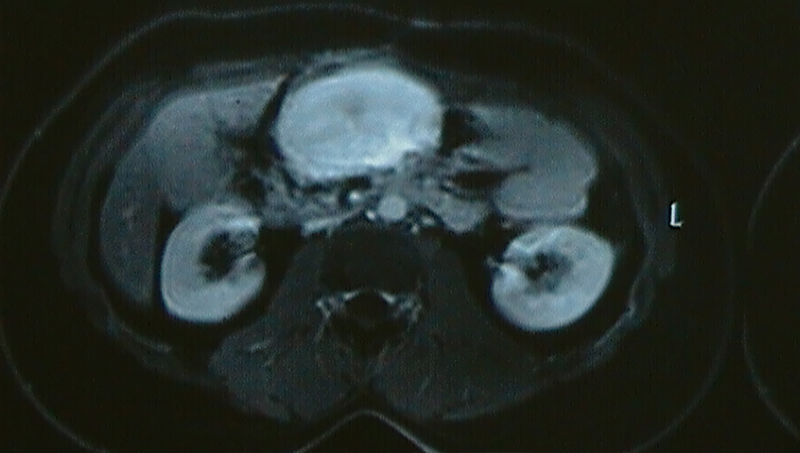
24 year old young man underwent a total proctocolectomy and coloanal anastomosis for colonic polyposis (Turcot’s syndrome). He developed a large central mesenteric tumor one year later which was causing intestinal obstruction. He was operated for the same. Tumor along with 2 feet of small intestine was removed followed by anastomosis of the small intestine. Final histopathological examination showed a desmoid tumor. Patient survived for more than 5 years after initial diagnosis and finally died of a brain tumor.
Tumors located in the central mesentery of small intestine (area between superior mesenteric artery & vein) are very difficult to operate due to the location, vascular nature, the large size they attain by the time they are diagnosed and large portion of small intestine involved. The surgery may have significant blood loss and result in removal of large segment of small intestine. The nature of these tumors could be Gastro Intestinal Stromal Tumor (GIST), Neuro Endocrine Tumor (NET), desmoid tumor, Lymphoma etcetera. These tumors may present with abdominal pain, weight loss, vomiting, abdominal distension, early satiety, intestinal obstruction, gastrointestinal bleeding (meleena – dark / blackish stools, massive bleeding per rectum, slow bleeding in stools causing anemia). Rarely they present as intestinal perforation or bleeding in the peritoneal cavity (hemoperitoneum).
The treatment is a carefully planned surgery wherein the major blood vessels are protected, as much portion of small intestine as possible is preserved while still doing a radical cancer surgery & blood loss is kept to a minimum. In some patients a multivisceral resection (removal of small intestine, large intestine, omentum and part of pancreas) is needed.
Due to the uncommon nature of these tumors very few surgeons have the reasonable exposure to handle these tumors. Dr. Kulkarni has operated 4 such patients so far, 2 large GISTs, 1 NET & 1 desmoid tumor.