Laparoscopic gastrectomy is commonly done for early gastric cancer, small gastric tumors or rarely for benign gastric obstructions. However it can be done for large gastric tumors provided requisite skills are there. These tumors include gastric adenocarcinomas, gastrointestinal stromal tumors (GIST) or Neuro endocrine tumors. We recently did one such patient which eventually turned out to be a GIST.
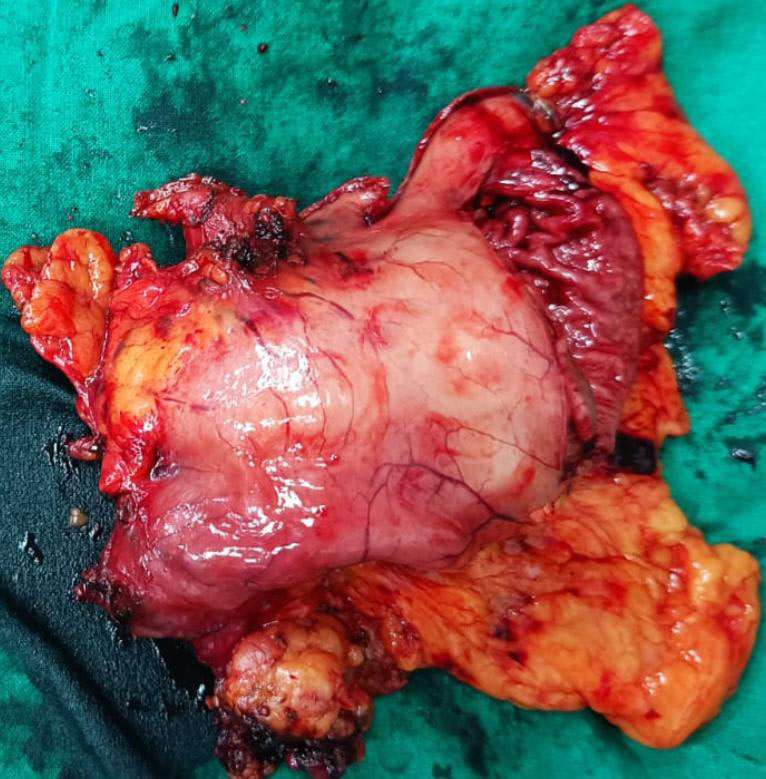
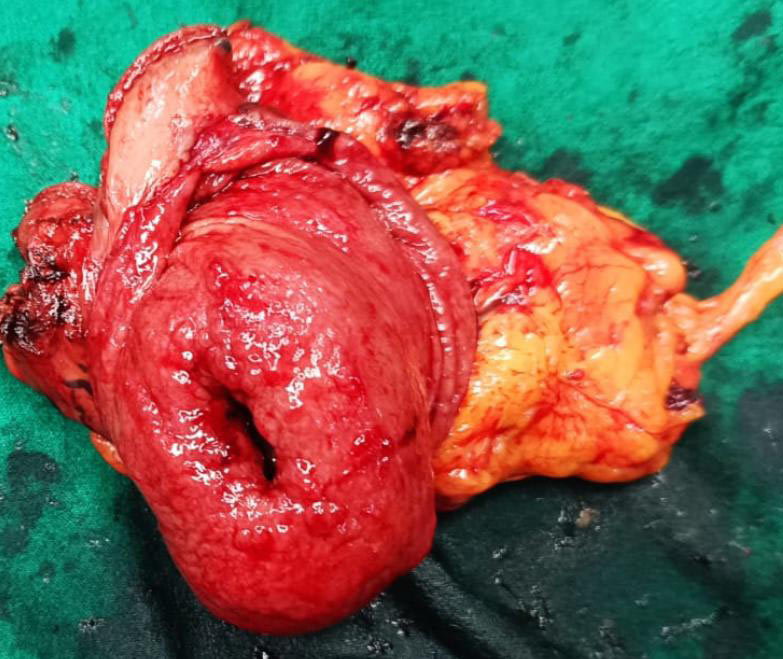
70 year old gentleman came with complaints of fullness of abdomen, vague abdominal discomfort and weight loss. He had a palpable upper abdominal lump. His old investigation s showed a gastric tumor that was gradually increasing in size over few years. His fresh investigations showed that the tumor had further grown, was ulcerated inside the stomach & was causing obstruction to passage of food from stomach to intestines. He also had gallstones & significant constipation. PET CT did not show any spread except a lymph node in the vicinity of tumor. Since patient needed a surgery (obstruction, ulceration, bleeding) and the tumor was resectable; he was subjected to surgery without biopsy. A laparoscopic distal radical gastrectomy (lymph node clearance) (image 1) was performed followed by gastrointestinal reconstruction. Simultaneously laparoscopic cholecystectomy was done for gallstones. Patient was sent home on day 6. The final histopathology was GIST. Based on the detailed histopathology, patient was started on oral chemotherapy.
Large GISTs / NETS & advanced gastric adenocarcinomas are usually not suitable for upfront surgery especially a laparoscopic one. These patients are initially treated with some form of chemotherapy and once they are reduced in size and spread; a laparoscopic or open surgery is performed. However we were able to perform laparoscopic gastrectomy in our patient with large GIST.