78 year old gentleman was transferred under our care from private nursing home. Papers revealed that he was admitted in the previous place with acute abdominal pain, severe sepsis and acute kidney injury. Urine infection was thought to be the cause based on blood and urine investigations. CT scan of abdomen and pelvis did not show requirement of surgical intervention. Patient initially responded to broad spectrum antibiotics only to deteriorate again. This time the treating team from original hospital opted for a diagnostic laparoscopy instead of a repeat CT scan. During laparoscopy surgeon a drain was placed in the abdominal cavity and patient was advised an exploratory laparotomy if there was no improvement. At this point family shifted the patient under our care.
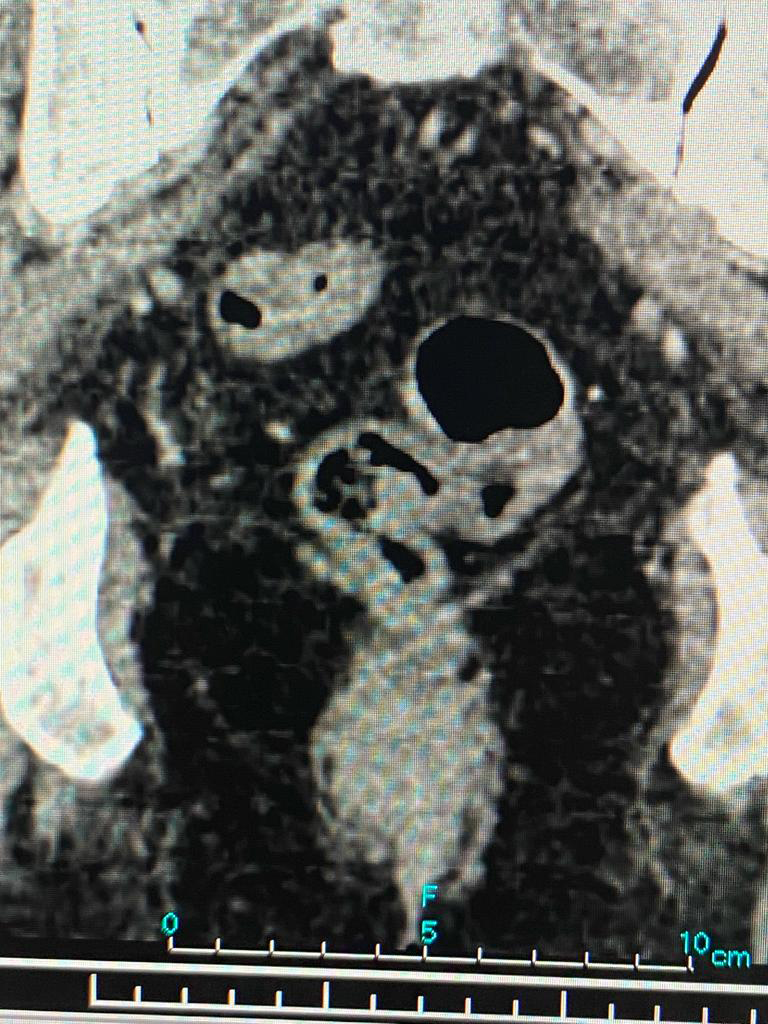
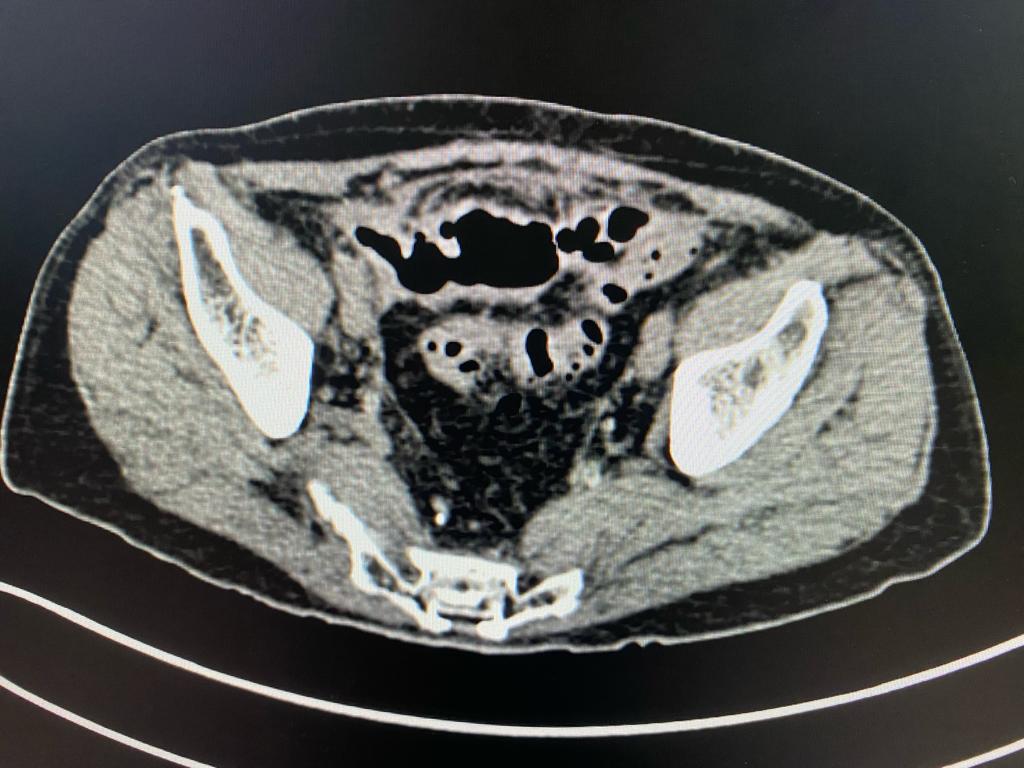
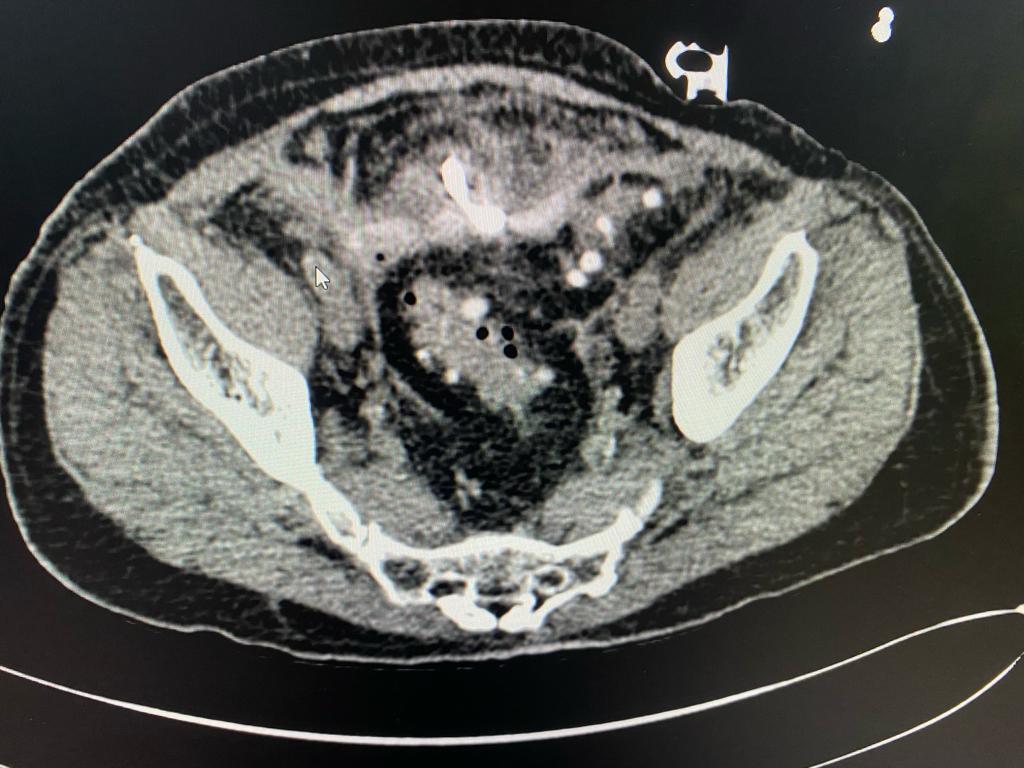
After admission, we reviewed the history, investigations, sequence of events and old CT scan. We suspected colonic diverticulosis with perforation as the original reason for sepsis. We repeated the CT scan of abdomen and pelvis which showed a pelvic abscess along with a sigmoid colonic diverticular phlegmon confirming diverticular perforation. The drain placed during previous laparoscopy was out of position. After a multidisciplinary meeting, treatment plan was charted out. The original drain was used to guide another drain deep in the pelvic abscess cavity under radiological guidance thus ensuring free drainage. The antibiotics were adjusted based on culture sensitivity of the intraabdominal pus. There were multiple highly resistant organisms and very few antibiotics were available for treatment. Hence the definitive surgery was deferred. Patient recovered and was sent home on intravenous antibiotics and drainage catheter.
Patient was closely monitored by our team. When the drainage reduced to near zero, the catheter was blocked and antibiotics were continued for a period of 4 weeks and then stopped. Coise monitoring showed that problem had not settled fully. Hence a temporary faecal diversion or colostomy (bringing large intestine on the skin surface to divert stool passage) was done. Patient was restarted on antibiotics and drainage catheter kept open. The whole aim was to buy time to reach the opportune moment when definitive surgery (sigmoid colon removal) could be done safely. Patient again settled clinically and antibiotics were stopped.
Patient was scheduled for the definitive surgery almost 6 weeks after the colostomy and almost 3 months after beginning of the problem. We still faced the issue of multiple resistant organisms and limited availability of antibiotics. The surgery was a laparoscopic assisted sigmoid Colectomy and small intestinal resection anastomosis. The colostomy was not taken down to protect the colonic anastomosis. Patient recovered well after surgery.


Points to remember