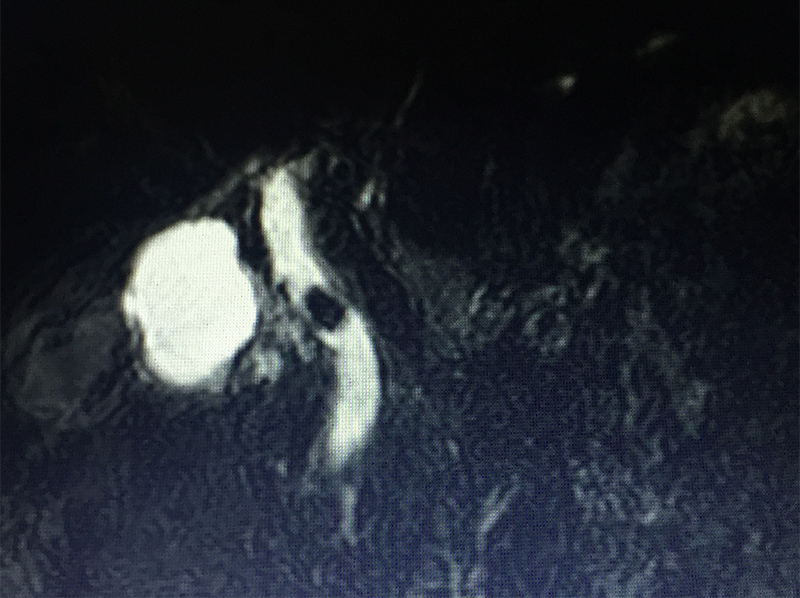
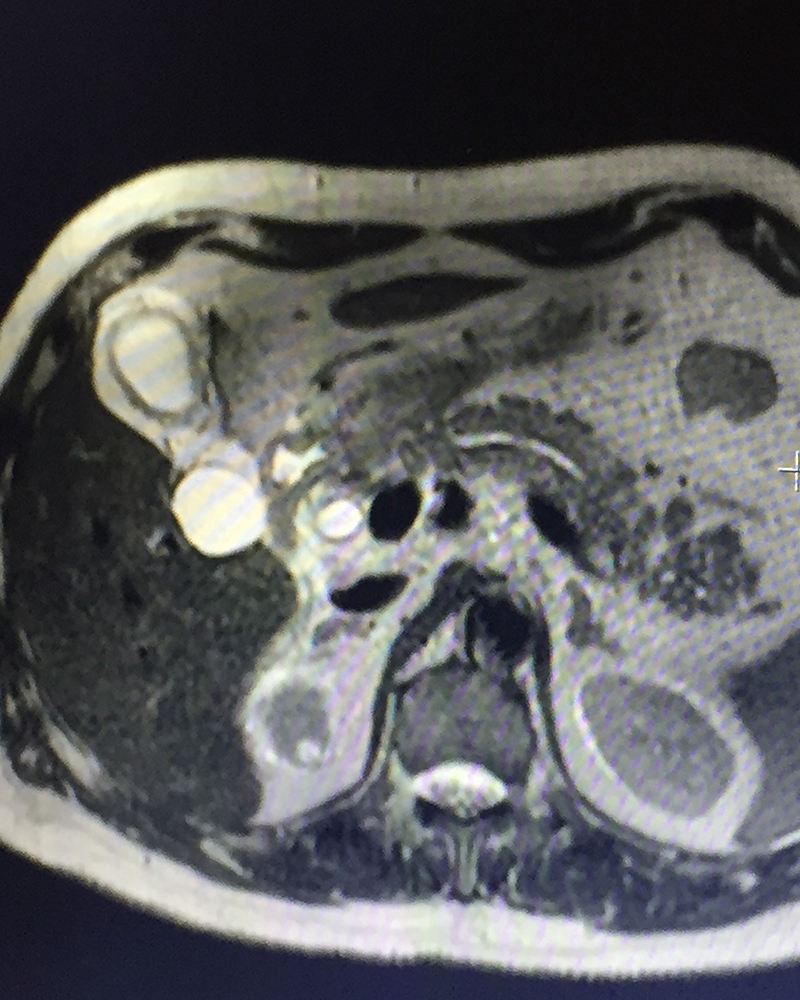
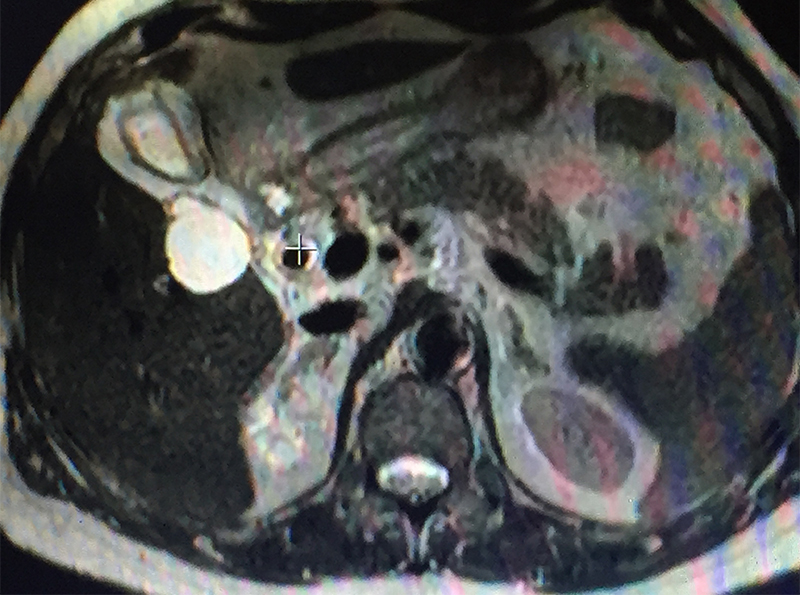
79 year old gentleman with diabetes, hypertension, cardiac problems, previous coronary bypass surgery and borderline renal function presented with acute abdominal pain in the right upper abdomen & periumbilical area, vomiting, abdominal bloating / distension and not passing gases. He had one episode of high grade fever too. Initial investigations (blood & abdominal sonography) showed evidence of infection (high leucocyte count & CRP), jaundice (raised bilirubin), biliary infection / inflammation – cholecystitis / cholangitis -- (raised SGOT / SGPT / alkaline phosphatase -- liver enzymes), mild pancreatitis (raised amylase / lipase –pancreatic enzymes) and worsening renal function (BUN / creatinine). The ultrasonography showed stones in the gall bladder with severe cholecystitis (gall bladder inflammation / swelling), large stones in the bile duct and pancreatitis (inflammation / swelling of pancreas). The patient was diagnosed with acute calculous cholecystitis, obstructive jaundice & cholangitis due to stones in the bile duct, acute biliary pancreatitis (pancreatitis caused by passage of stone / obstruction of mouth of the common channel of bile & pancreatic duct). The vomiting, dehydration & infection had caused acute injury to the already compromised kidney (due to diabetes & hypertension) leading to further worsening of the renal function. A MRCP (MRI examination of biliary / pancreatic ducts) & IV contrast MRI abdomen was done to confirm the diagnosis. The pancreatitis was fortunately mild on MRI.
The patient was unstable, had low blood pressure, needed supports to maintain it; thus indicating that he was in severe biliary sepsis. Patient needed an early ERCP (endoscopy of biliary & pancreatic duct) and removal of stone with stent insertion in the bile duct to control the sepsis. Since patient was on anticoagulation / antiplatelet medications (aspirin & ticagrelor, there was limitations in doing the endoscopic procedure, which involved an internal cut over the mouth of the bile duct (sphincterotomy). This would cause severe uncontrolled bleeding due to the drugs effect. Hence the procedure was modified and an ERCP & only stent insertion was done to drain the infected bile duct. Frank pus drained out, which was sent for culture and antibiotic sensitivity test. This drainage helped to tide over the infection along with antibiotics and bought us time to wait till the effect of antiplatelet drugs was over. The biliary drainage partially controlled the infection and stabilized the patient. Blood pressure supports reduced, pancreatitis settled and jaundice subsided. 4 days later a repeat ERCP was done, sphincterotomy was done without any bleeding and 2 large stones were removed. Stent was reinserted for assisting the bile drainage. Antibiotics were adjusted as per the bile culture report.
However infection could not be completely controlled & the creatinine remained high due to infection in the gall bladder. The gall bladder removal (laparoscopic cholecystectomy) was completed 48 hours after the ERCP. Post surgery patient improved dramatically and was shifted out of the ICU. He was discharges 7 days after the surgery.
Gall stones is a seemingly innocuous problem for many and is often taken lightly. This is because a large subset of patients with gall stones remain asymptomatic for a long period of time and sometimes throughout the life. However when they become symptomatic & / or cause complications like biliary infection (cholangitis / cholecystitis) & pancreatitis especially in elderly patients with multisystem comorbid problems like diabetes, hypertension, cardiac disease, previous surgery, renal failure; then management becomes extremely difficult as was seen in our patient.
To know more about gall stones & its management click here.